Session: (0554–0592) Spondyloarthritis Including Psoriatic Arthritis – Treatment Poster I
0590: Effect of Deucravacitinib Treatment on Disease Activity–Associated Plasma Biomarkers in Patients With Active Psoriatic Arthritis: Results From 2 Phase 3 Studies
Vinod Chandran1, Oliver FitzGerald2, Philip J. Mease3, Lihi Eder4, Jose Scher5, Christopher Ritchlin6, Dafna D. Gladman7, Walter P Maksymowych8, Coryandar Gilvary9, Aditi Basu Bal9, Eleni Vritzali10 and Jinqi Liu9, 1Division of Rheumatology, Departments of Medicine and Laboratory Medicine and Pathobiology, University of Toronto, and Gladman Krembil Psoriatic Arthritis Research Program, Krembil Research Institute, University Health Network, Toronto, Canada, 2UCD, Dublin 6, Dublin, Ireland, 3Department of Rheumatology, Providence-Swedish Medical Center and University of Washington, Seattle, WA, 4University of Toronto, Toronto, ON, Canada, 5New York University School of Medicine, New York, NY, 6University of Rochester Medical Center, Canandaigua, NY, 7Schroeder Arthritis Institute, Krembil Research Institute, Toronto Western Hospital, Division of Rheumatology, Toronto, ON, Canada, 8Department of Medicine, University of Alberta, Edmonton, AB, Canada, 9Bristol Myers Squibb, Princeton, NJ, 10Bristol Myers Squibb, Boudry, Switzerland
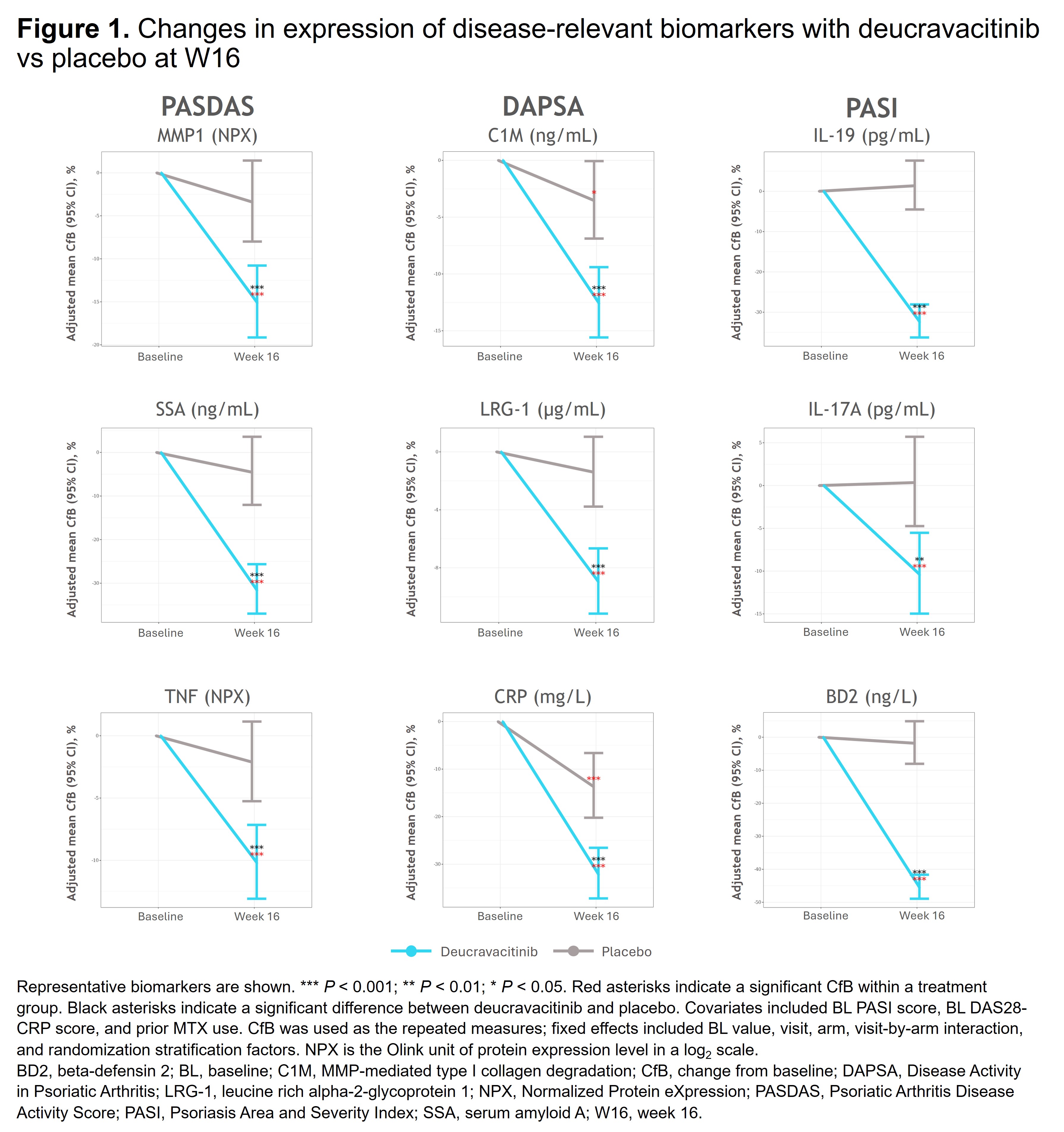
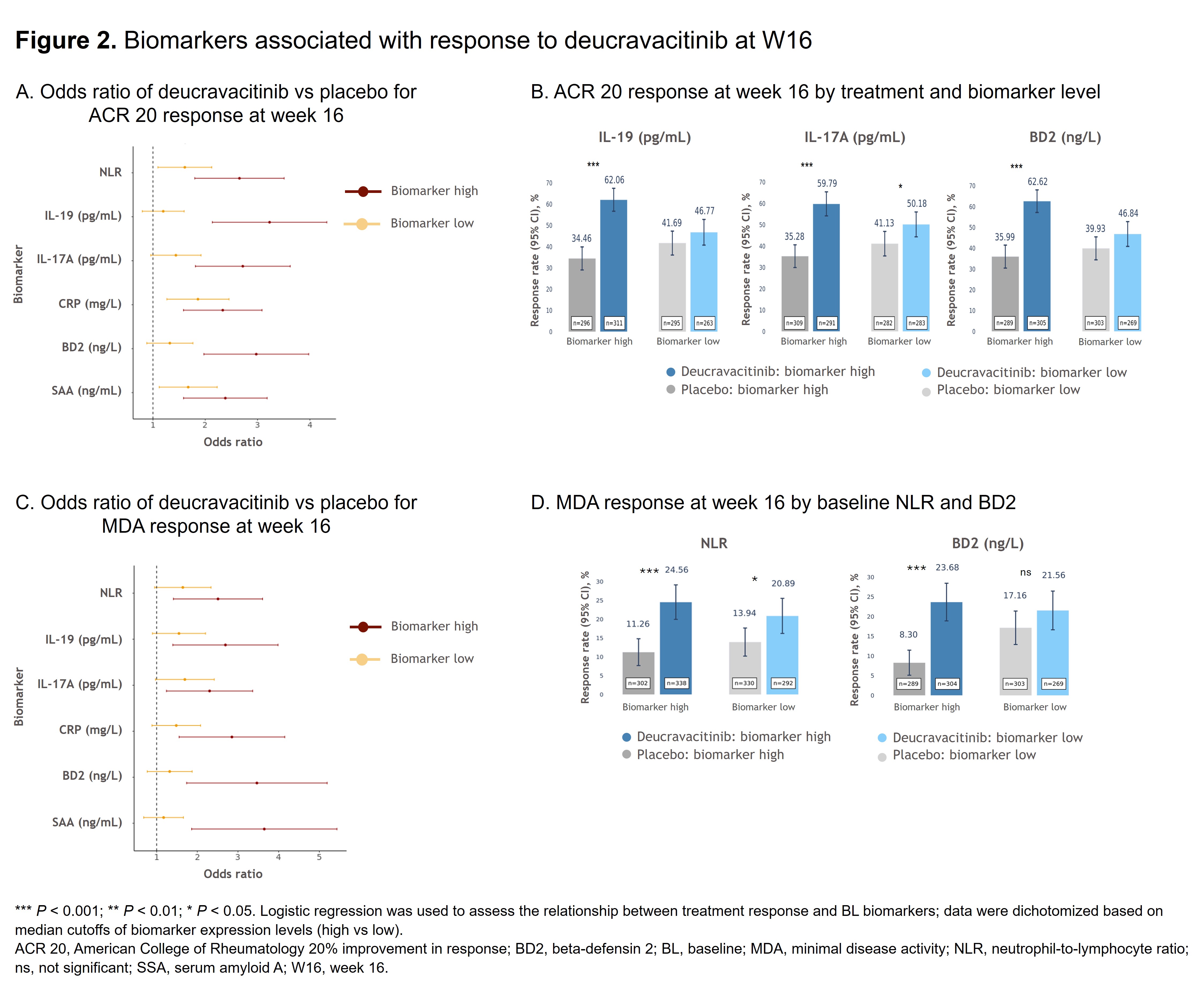
Background/Purpose: Understanding how treatments affect disease-relevant biomarker expression is essential for advancing targeted therapies. Deucravacitinib, an oral, selective, allosteric tyrosine kinase 2 (TYK2) inhibitor, has demonstrated superior efficacy in the placebo (PBO)-controlled phase 3 POETYK PsA-1 (NCT04908202) and PsA-2 (NCT04908189) studies. This pooled post hoc analysis of the POETYK PsA studies aimed to identify biomarkers reflecting clinically relevant factors potentially associated with poor prognosis in PsA and to evaluate associations among these biomarkers, deucravacitinib treatment, and clinical responses. Methods: Spearman correlations between 48 PsA and immune response–related biomarkers and PsA disease activity (PASDAS, DAPSA, PASI) at baseline (BL) and W16 were performed. Pharmacodynamic effects of deucravacitinib on biomarkers were analyzed using a mixed effects model to show covariate-adjusted change from BL for disease activity and Patient Global Assessment of Pain (Pain). Logistic regression was used to assess the relationship between BL biomarkers (eg, CRP, neutrophil-to-lymphocyte ratio [NLR]) and ACR 20 response, minimal disease activity (MDA) response, and modified Sharp-van der Heijde (mSvdH) total score (radiographic progression [defined as change of mSvdH > 0]; evaluated in POETYK PsA-1 only); covariates included BL BMI and prior MTX use. mSvdH nonprogression was evaluated using a stratified Cochran-Mantel-Haenszel test with BL csDMARD use as the stratification factor. Results: Deucravacitinib significantly reduced disease activity–associated biomarkers, including those impacting skin (eg, IL-19, IL-17A, BD2) and joint (eg, CRP, C1M, LRG-1, MMP1, SAA, TNF) manifestations vs PBO (Figure 1). Patients treated with deucravacitinib were more likely to achieve ACR 20 and MDA response vs PBO at W16 in those with high (≥ median) BL NLR, IL-19, IL-17A, CRP, BD2, and SAA (Figure 2A,C). Response rates for ACR 20 and MDA were higher with deucravacitinib vs PBO at W16, with significant differences observed in patients with high (≥ median) BL IL-19, IL-17A, and BD2 for ACR 20 (Figure 2B) and high BL NLR (≥ 2.81) or high BD2 levels (≥ 7185 ng/L) for MDA (Figure 2D). Deucravacitinib reduced pain-associated biomarkers (eg, CRP, C1M, MMP3, TNF, ICAM-1) vs PBO at W16. Given the clinical relevance of CRP, additional analyses in patients with high BL CRP (≥ 3 mg/L) showed that deucravacitinib significantly reduced Pain score vs PBO as early as W4 (P < 0.01) with sustained reduction at W16 (P < 0.001), provided a greater reduction in mSvdH total score (PBO corrected) vs those with normal BL CRP, and led to reduced radiographic progression vs PBO at W16 (21.1% vs 30.6%; P < 0.05). Conclusion: Deucravacitinib significantly reduced PsA disease–associated biomarkers in patients with elevated BL biomarkers (eg, CRP, NLR), which may be indicative of severe disease and poor prognosis, and improved efficacy outcomes for multiple disease domains, including radiographic progression. These data provide biological evidence for deucravacitinib as a potential new oral PsA therapy that may benefit patients with severe and difficult-to-treat disease.