Session: (0430–0469) Rheumatoid Arthritis – Diagnosis, Manifestations, and Outcomes Poster I
0445: GLP-1 Receptor Agonists Reduce Mortality and Cardiovascular Events in Patients with Rheumatoid Arthritis
Sunday, October 26, 2025
10:30 AM - 12:30 PM Central Time
Location: Hall F1
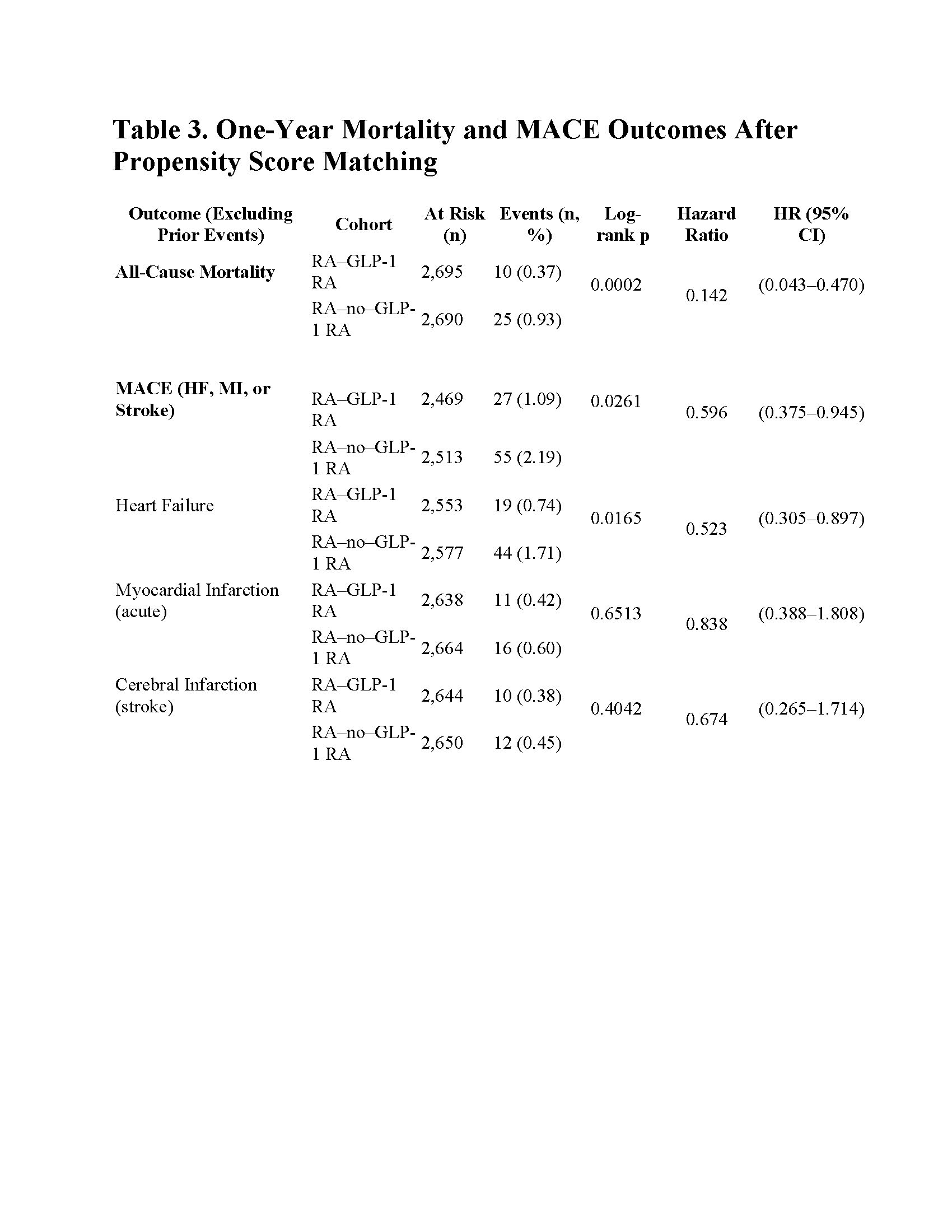
This table summarizes 1-year incidence of all-cause mortality and major adverse cardiovascular events (MACE) among RA–GLP-1 RA versus RA–no–GLP-1 RA cohorts, post–propensity score matching.
Thomas Jefferson University Philadelphia, Pennsylvania, United States
Disclosure(s): No financial relationships with ineligible companies to disclose
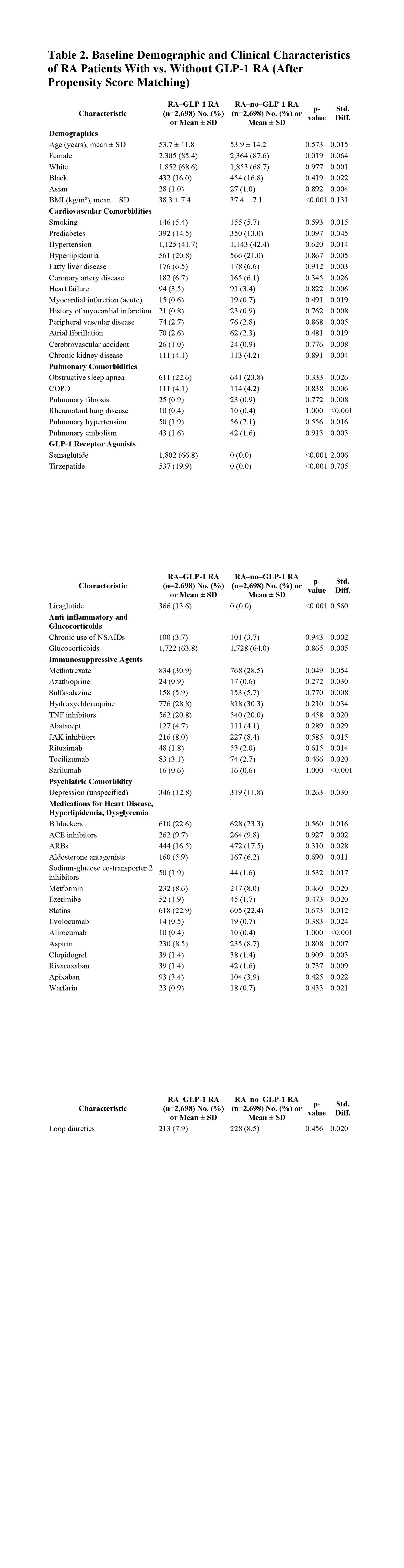
Background/Purpose: Obesity significantly increases cardiovascular morbidity and mortality in rheumatoid arthritis (RA), yet effective strategies for managing obesity-related risks in this population remain limited. Glucagon-like peptide-1 receptor agonists (GLP-1 RAs) offer substantial cardiometabolic benefits in diabetic populations, but their effects in obese RA patients without diabetes are not well defined. This study investigated whether GLP-1 RA therapy reduces one-year all-cause mortality and major adverse cardiovascular events (MACE) in non-diabetic obese RA patients. Methods: This retrospective cohort study utilized the TriNetX platform, selecting adults (≥18 years) with RA, obesity (BMI ≥30 kg/m²), and no history of diabetes mellitus. Patients initiating GLP-1 RA treatment (semaglutide, liraglutide, tirzepatide) were propensity score–matched (1:1) with RA controls not receiving GLP-1 RA therapy, balancing demographics, BMI categories, cardiovascular comorbidities, immunosuppressive therapies, and cardiometabolic medications. The primary endpoint was all-cause mortality at one year; secondary outcomes included new-onset MACE (heart failure, myocardial infarction, stroke) (Table 1) Results: The matched analysis included 2,698 patients per group (Table 2). GLP-1 RA treatment was associated with significantly reduced one-year all-cause mortality compared to matched controls (0.37% vs. 0.93%; HR, 0.14; 95% CI, 0.04–0.47; p=0.0002). Additionally, MACE incidence was significantly lower in the GLP-1 RA group (1.09% vs. 2.19%; HR, 0.60; 95% CI, 0.38–0.95; p=0.026), driven primarily by fewer heart failure events (0.74% vs. 1.71%; HR, 0.52; 95% CI, 0.31–0.90; p=0.017). Myocardial infarction and cerebrovascular infarction rates were not significantly different between groups. (Table 3) Conclusion: In obese, non-diabetic RA patients, GLP-1 RA therapy significantly reduced one-year all-cause mortality and cardiovascular events, particularly heart failure. These results highlight GLP-1 RAs as a promising therapeutic option for cardiometabolic risk reduction in RA. Prospective trials are warranted to confirm these findings.

.jpg)