Session: (0430–0469) Rheumatoid Arthritis – Diagnosis, Manifestations, and Outcomes Poster I
0449: Consistency of CDAI Low-Disease Activity (LDA) Outcomes with Time in a Large US Registry: Association With Patient-Reported Clinical Outcomes and Measures of Quality of Life
Background/Purpose: Low disease activity has been identified as a treatment goal for the treatment of RA. A single
center RA registry (BRASS) reported a difference in outcome in RA pts who achieved remission
versus low disease activity 1
. When LDA was subdivided between very low disease activity
(VLDA >2.8< 6) and LDA scores from >6< 10 and remission CDAI < 2.8 there were also
differences in outcome between those pts in VLDA versus LDA suggesting that the threshold for
“true” LDA should be lowered. This study further examined this issue in a large US RA registry Methods: Population: RA patients from the US-based CorEvitas RA registry (122 private sites, 21
academic sites).
Inclusion: Patients (pts) on a biologic (baseline) and a 1-year (9-15 mos) and 2-year (21-27
mos). Target defined as LDA (CDAI ≤10). Pts at one year divided into 1) Consistently on target
2) Lose target; 4) Gain Target 5) Consistently not at target. The sub-population consistently on
target were divided into remission (≤2.8), very low disease activity (VLDA: >2.8 and ≤6) or high
LDA (HLDA >6 and ≤10) at one year. Baseline characteristics, HAQdi, pain and fatigue at 1
and 2 years were compared across groups. Linear regression analysis examined these outcomes
at 1 year adjusting for age, gender, RA duration, Charlson Comorbidity Index(CCI) and CDAI
(all at baseline). Results: 13,513 pts with baseline visits between 2001-2023 were included in the analysis. 5,570 (41.4%)
“consistently at target”,1,330 (9.8%) “Flare/Lose Target”, 2,542 (18.8%) “Gain Target” , and
4,071 (30.13%) “Consistently not at Target” .
“Consistently at Target”, 2,690 (48.3%) pts were classified at one year as “Remission” , 1,694
(30.4%) VLDA , and 1,186 (21.3% ) HLDA. Baseline characteristics are seen in Table 1.
Groups with CDAI > 10 at 1-year had worse functional outcome in HAQdi, pt reported pain
and fatigue at both year 1 and 2 than the two groups who had CDAI < 10 at 1-year in both
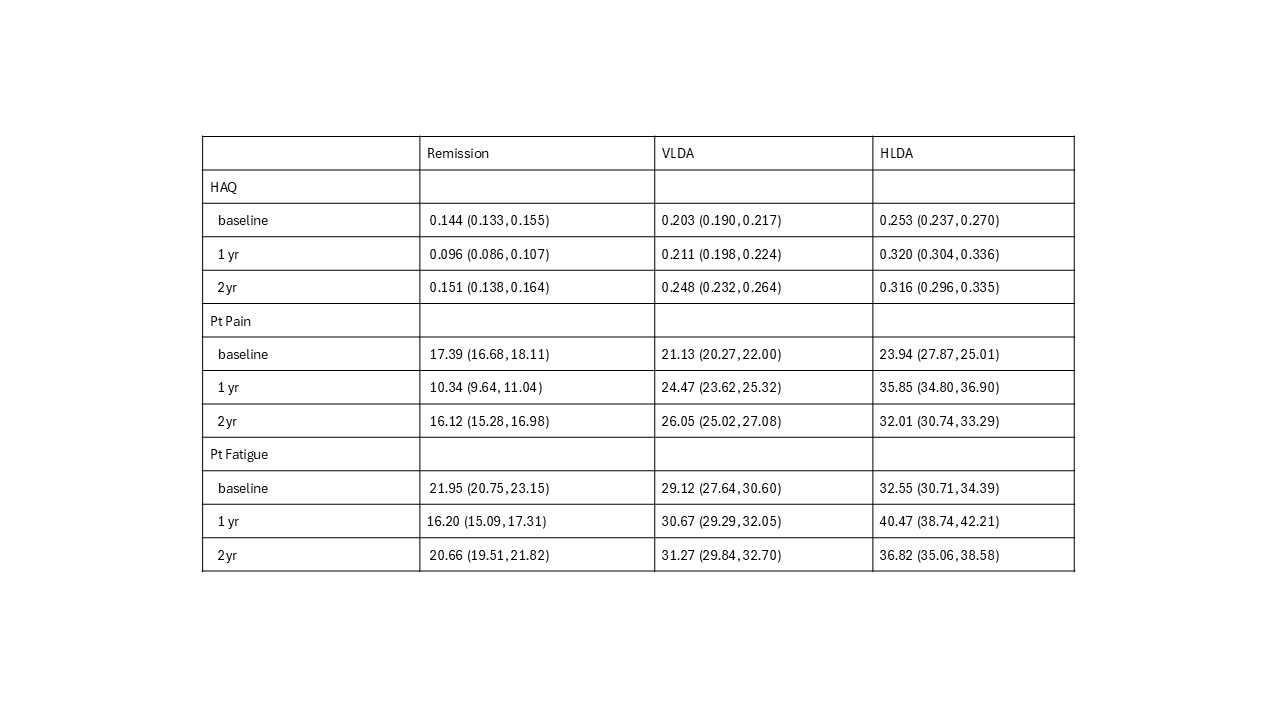
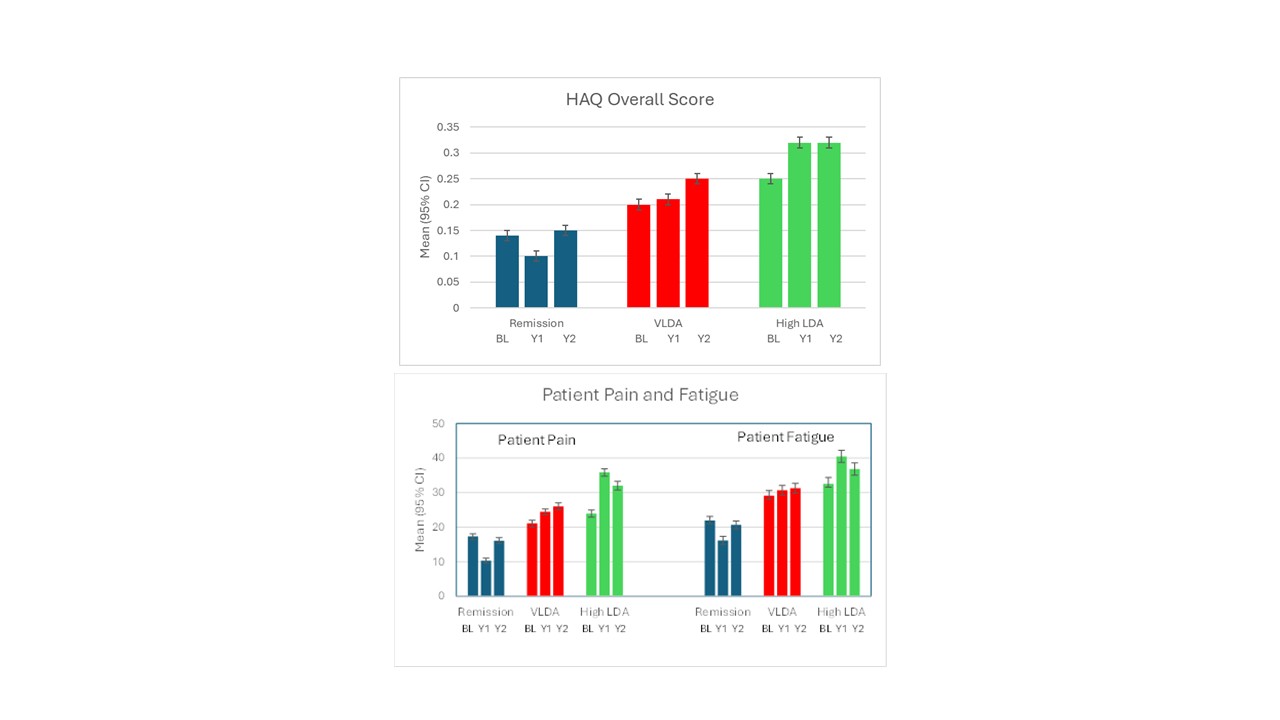
unadjusted and adjusted models (p< 0.01).Within the consistently at target group, HLDA (CDAI >6 and < 10) pts had significantly worse
functional outcome on HAQdi, pt reported pain, and fatigue than the VLDA and remission
groups at year 1 and 2 years (p< 0.01). The VLDA patients had worse functional outcome than
the remission group (p< 0.01). Figure 1. Conclusion: This very large observational study demonstrates that there are meaningful patient-reported
differences in the consistency of the categories of “LDA” response including HAQdi, pt pain and
fatigue, that are significantly associated with LDA subcategory status (remission, VLDA and
HLDA). These significant and meaningful differences in “LDA status” with treatment are lost
when considering only a broad definition of LDA. Our results show that the LDA cutpoint
should be lowered from CDAI ≤10 to CDAI ≤6 for a more realistic evaluation of patient
functional outcomes when judging what is now called LDA.

.jpg)