1208: Neutrophil Activation in Juvenile Dermatomyositis: Associations with Muscle Function and Disease Progression
Monday, October 27, 2025
10:30 AM - 12:30 PM Central Time
Location: Hall F1
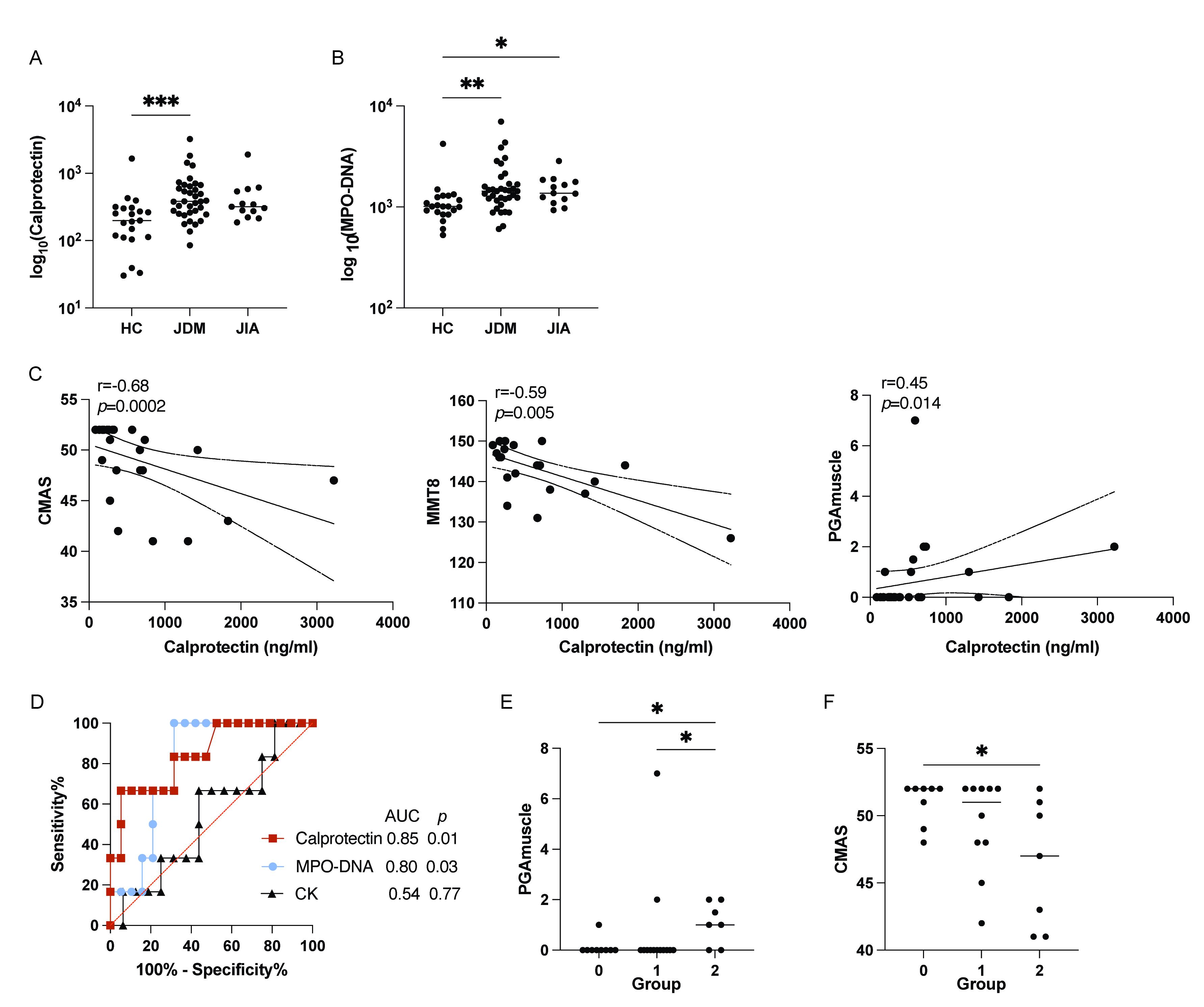
Figure 1. Neutrophil activation levels in JDM and associations with disease activity markers. (A, B) Levels of calprotectin (A) and MPO-DNA (B) in plasma among different groups. (C) Correlation of calprotectin with CMAS, MMT8, and PGA muscle score. (D) ROC curves comparing the performance of calprotectin, MPO-DNA and CK levels in distinguishing active from remission states in JDM patients based on CMAS. Active disease was defined as a CMAS ≤ 47. (E-F) PGA muscle scores (E) and CMAS (F) in JDM patients stratified into three groups based on neutrophil activation marker levels. Group 0: low level of both calprotectin and MPO-DNA; Group 1: elevated level of either biomarker; Group 2: elevated levels of both biomarkers.
Statistical analyses by Kruskal-Wallis test, Spearman correlation and Mann-Whitney U test with * p<0.05, ** p<0.01, and *** p<0.001.
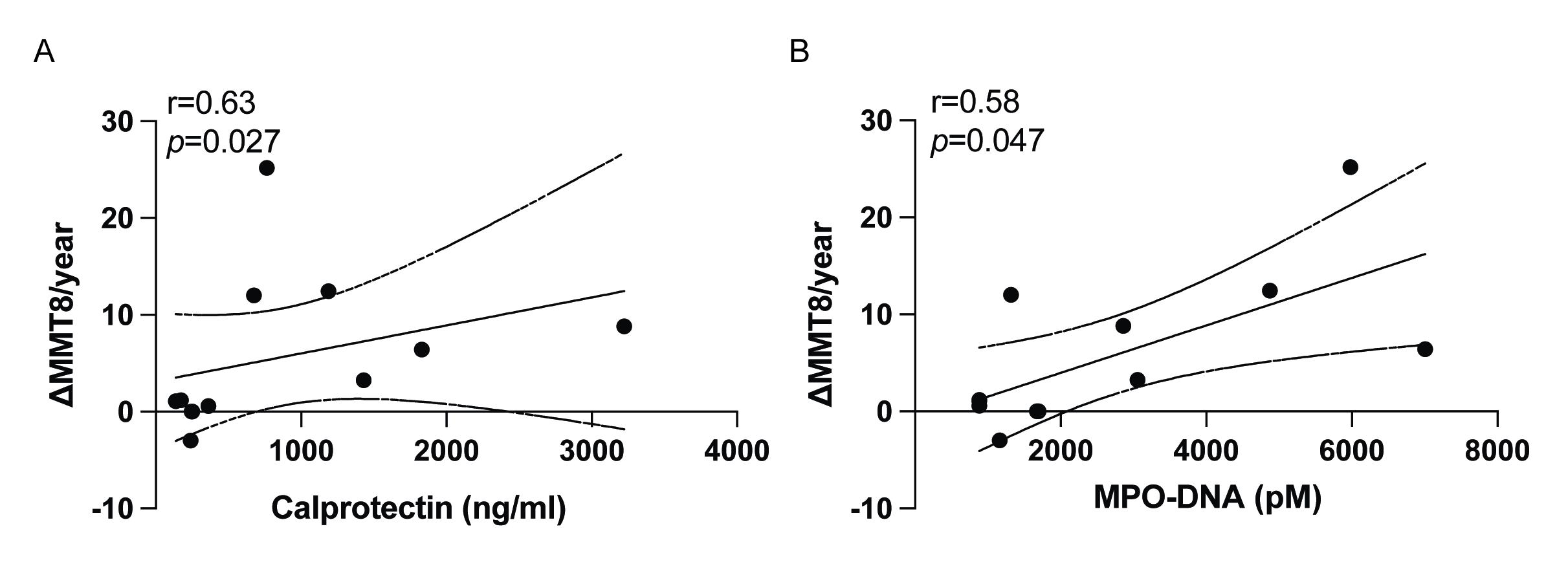
Figure 2. Correlations of neutrophil activation markers and disease progression in JDM. (A-B) Correlation analysis between plasma levels of calprotectin (A) and MPO-DNA (B) and MMT8 progression in JDM.
Statistical analyses by Spearman correlation.
University of Washington Seattle, Washington, United States
Disclosure(s): No financial relationships with ineligible companies to disclose
Background/Purpose: Juvenile dermatomyositis (JDM) is an inflammatory vasculopathy characterized by muscle weakness and systemic inflammation. This study aimed to investigate the clinical utility of neutrophil activation markers, specifically calprotectin (S100A8/A9) and myeloperoxidase (MPO)-DNA complexes, as potential biomarkers for muscle inflammation and predictors of long-term outcomes in JDM. Methods: Plasma levels of calprotectin and MPO-DNA were quantified using ELISA in JDM (n = 36), juvenile idiopathic arthritis (JIA, n = 13), and healthy controls (HCs, n = 21). Disease severity and muscle function were assessed using the Childhood Myositis Assessment Scale (CMAS), Physician Global Assessment (PGA), and Manual Muscle Testing 8 (MMT8). Results: JDM patients exhibited significantly higher plasma calprotectin and MPO-DNA levels as compared to HCs (p=0.0008 and p=0.0048, respectively) (Figures 1A-B). Calprotectin levels correlated with muscle function scores (CMAS r=-0.682, p=0.0002; MMT8 r=-0.59, p=0.005; and PGA muscle scores r=0.452, p=0.014) (Figure 1C). ROC analysis demonstrated that baseline calprotectin and MPO-DNA levels could distinguish active disease with high accuracy (AUC = 0.85 and 0.80, respectively) (Figure 1D). Further stratification showed that patients with elevated levels of both markers had significantly worse disease activity and muscle involvement (Figures 1E-F). Notably, higher baseline levels of these markers correlated with improved MMT8 scores over time (r=0.634, p=0.027; r=0.582, p=0.047) (Figures 2A-B), indicating a predictive role in muscle recovery. Conclusion: Calprotectin and MPO-DNA represent promising biomarkers for muscle inflammation and functional outcomes in JDM. These results suggest that neutrophil activation plays a key role in JDM pathogenesis and may provide insights into disease monitoring and treatment strategies.