Disclosure(s): No financial relationships with ineligible companies to disclose
Background/Purpose: Interstitial lung disease (ILD) is a prevalent feature among patients suffering from connective tissue diseases (CTD), associated with considerable morbi-mortality. Nonetheless, this complication is still poorly defined in our field.
The purpose of this work is to assess the main characteristics of CTD-ILD in our area. Methods: An ambispective regional registry (NIRRVANA Registry: Neumopatía Intersticial en Reumatología Registro VAsco-NAvarro) of CTD-ILD was conducted in the Basque Country and Navarre, Spain. Adult patients with ILD associated with aPLS, IIM, MCTD, RA, sarcoidosis, SjS, SLE, SSc, UCTD and vasculitis (classification criteria or clinician's judgment) were included, as well as patients meeting criteria for IPAF.
Data on demographics, clinical, radiological and anatomo-pathological features, laboratory results, and outcomes were collected.
Statistical analyses were conducted using standardized tests. Results: One hundred and thirty-one patients were indentified (87 female, 44 male), with a median disease duration of 6.66 (2.72-13.49) years for CTDs.
RA (26.7%), followed by IIM (16.8%) and SSc (16.8) were the most frequent CTDs, while NSIP and IUP, for ILDs, were evident in equal proportion (29.8%) in this sample. Patients with NSIP were more frequent in the SSc and UCTD groups. UIP and OP were more common in the RA and IIM (specifically, ASS) groups, respectively. LIP was identified in only one case of SjS.
Fifty-six (42.7%) patients were diagnosed with CTD prior to ILD, 44 (33.6%) patients had CTD and ILD diagnoses concurrently, and 31 (23.7%) patients were diagnosed with ILD prior to CTD.
Details on both CTD and ILD identified, as well as demographic and clinical features, and main complementary studies performed, are collected in “Table 1”.
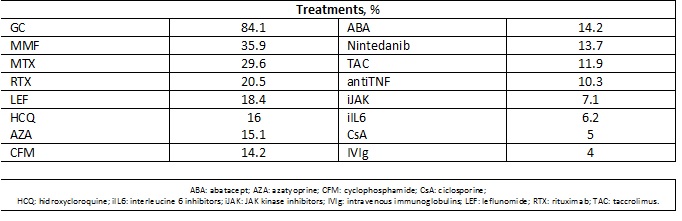
Glucocorticoids (GC) were used in 84.1% of the patients (mean initial oral dose 21.3mg per day, mean actual oral dose 2.3mg per day; 38.9% reached complete withdrawal of GC). Mycophenolate (MMF) and methotrexate (MTX) were the most commonly used immunosuppressants (IS). 48.4% of the patients needed ≥2 IS. Antifibrotics were needed in 13.7% of the patients. Regarding other treatments used in the NIRRVANA Registry, these are summarized in “Table 2”.
After 4.48 (2.2-9) years of median ILD duration, 16.8% patients showed improvement, with total resolution of ILD in 2 cases; stabilization was observed in 50.6% and progression in the remaining 32.6% cases. Of this latter group, 3 patients underwent pulmonary transplant, after a mean follow-up of 5.3 years, and 1 of them died in the context of acute respiratory failure and anasarca. Conclusion: ILD is a common but yet misunderstood complication of CTDs. The NIRRVANA Registry aims to deepen our understanding of the primary characteristics of these complications within a specific Spanish region, which will hopefully lead to improved management in the future. Ending of cross-sectional phase, a longitudinal follow-up of this registry, which is currently in progress, will provide with additional and relevant data towards achieving such goal.

.jpg)