Department of Medicine and Therapeutics, The Chinese University of Hong Kong Hong Kong, Hong Kong
Disclosure information not submitted.
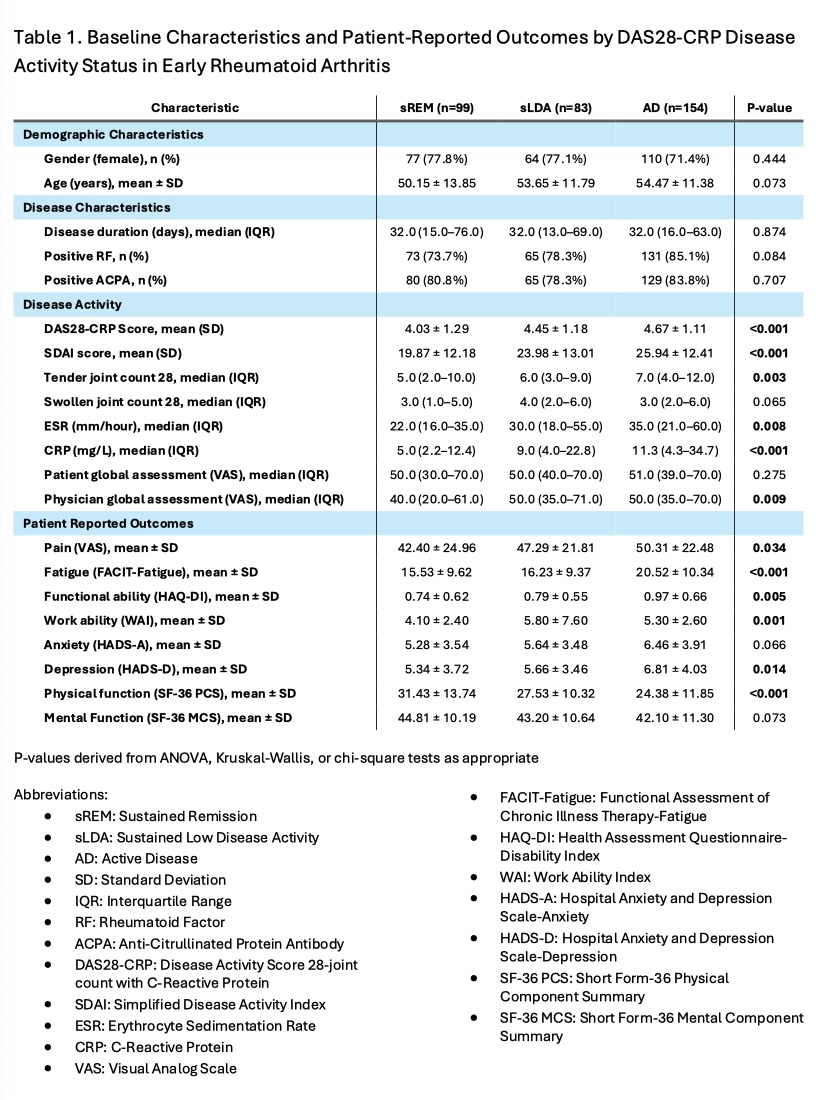
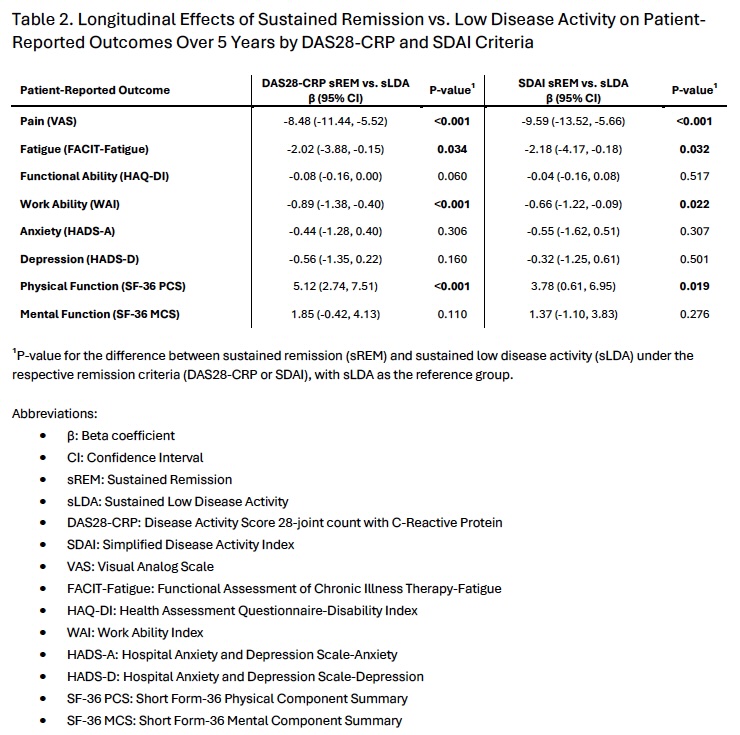
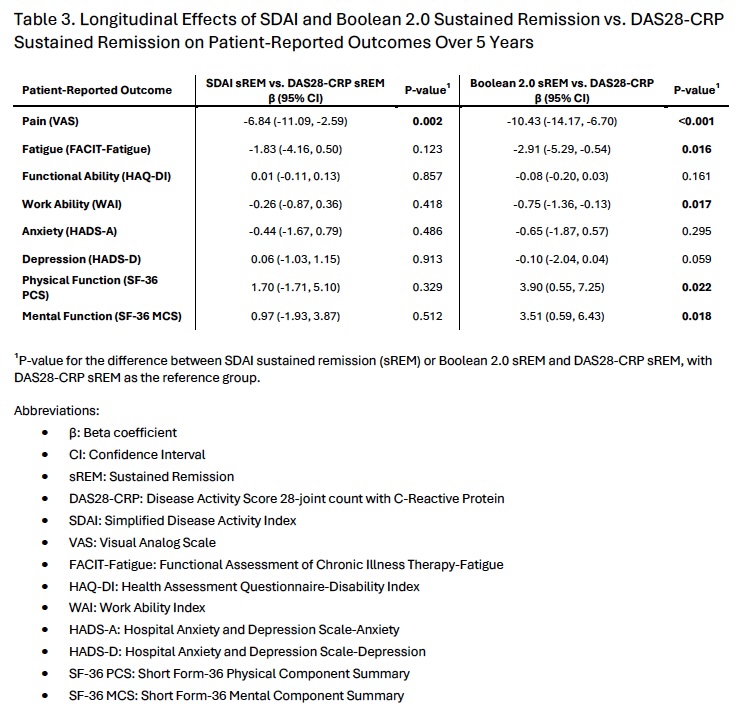
Background/Purpose: This study compared the impact of achieving early sustained remission (sREM) versus early sustained low disease activity (sLDA) on patient-reported outcomes (PROs) after 5 years in early rheumatoid arthritis (RA) patients, according to DAS28-CRP, SDAI, and Boolean 2.0 remission criteria. It also assessed PRO differences among patients achieving sREM across these criteria. Methods: Data were analyzed from 336 early RA patients (symptom onset < 2 years) in the Clinical Rheumatology Systematic Treat-to-Target in Asia Leadership (CRYSTAL) study who completed 5-year follow-up. Patients were classified into sREM, sLDA, or active disease (AD) groups based on DAS28-CRP and SDAI criteria, and sREM or AD for Boolean 2.0, at 6, 9, and 12 months. PROs, including fatigue (FACIT-Fatigue), functional disability (HAQ-DI), joint pain (VAS), anxiety and depression (HADS), work ability (WAI), and health-related quality of life (SF-36 physical [PCS] and mental [MCS] components), were evaluated over 5 years. Generalized estimating equations (GEE) models, adjusted for age, gender, and baseline disease activity, compared PROs between sREM and sLDA groups for DAS28-CRP and SDAI, and among sREM groups across DAS28-CRP, SDAI, and Boolean 2.0 criteria. Results: Of 336 patients, 99 (29%) achieved DAS28-CRP sREM, 38 (11%) SDAI sREM, and 36 (11%) Boolean 2.0 sREM, with 27 (8%) achieving sREM across all three criteria. Compared to DAS28-CRP sLDA, the DAS28-CRP sREM group had significantly better PROs in pain (β = -8.48, p < 0.001), fatigue (β = -2.02, p = 0.034), work ability (β = -0.89, p < 0.001), and SF-36 PCS (β = 5.12, p < 0.001) at year 5. Similarly, the SDAI sREM group outperformed SDAI sLDA in pain (β = -9.59, p < 0.001), fatigue (β = -2.18, p = 0.032), work ability (β = -0.66, p = 0.022), and SF-36 PCS (β = 3.78, p = 0.019). No significant differences were observed in functional disability, anxiety, depression, or SF-36 MCS for either comparison. All patients achieving SDAI or Boolean 2.0 sREM also achieved DAS28-CRP sREM. Compared to DAS28-CRP sREM (n = 99), SDAI sREM (n = 38) was associated with significantly lower pain (β = -6.84, p = 0.002) but no other PRO differences. Compared to DAS28-CRP sREM, Boolean 2.0 sREM group (n = 36) had better PROs in pain (β = -10.43, p < 0.001), fatigue (β = -2.91, p = 0.016), work ability (β = -0.75, p = 0.017), SF-36 PCS (β = 3.90, p = 0.022), and SF-36 MCS (β = 3.51, p = 0.018) after 5 years, but not in functional disability, anxiety, or depression. Conclusion: Early sustained remission, as defined by DAS28-CRP and SDAI criteria, is associated with significantly better pain, fatigue, work ability, and physical health-related quality of life compared to sustained low disease activity in early RA patients over 5 years. DAS28-CRP sREM is less stringent, as all patients achieving SDAI or Boolean 2.0 sREM also met DAS28-CRP criteria. However, SDAI sREM is associated with lower pain, and Boolean 2.0 sREM offers broader PRO benefits compared to DAS28-CRP sREM. These findings highlight the importance of early tight disease control using stricter criteria like SDAI or Boolean 2.0 to maximize long-term patient outcomes in early RA.