Session: (2227–2264) Rheumatoid Arthritis – Diagnosis, Manifestations, and Outcomes Poster III
2235: Proportion of Early Rheumatoid Arthritis Patients with Improved, Stable, or Worsened Lung Function Over 1-Year: Results from a Multicenter, Prospective Cohort Study
University of Michigan Ann Arbor, Michigan, United States
Disclosure(s): Caribous Pharmaceuticals: Consultant (Terminated, June 6, 2025)
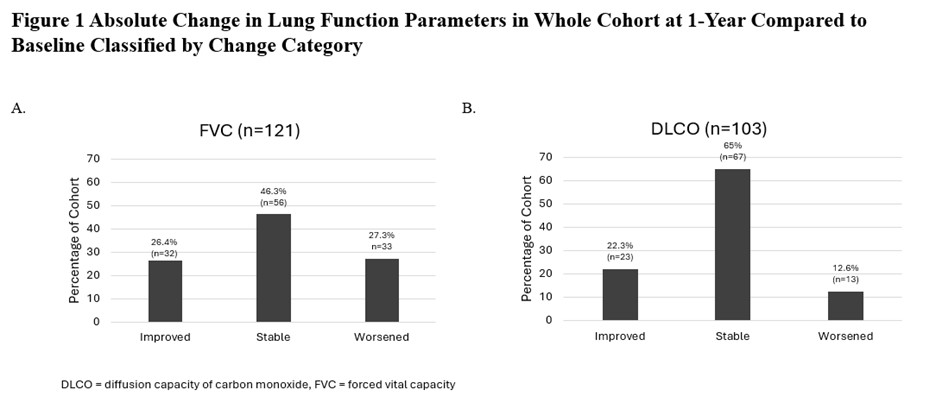
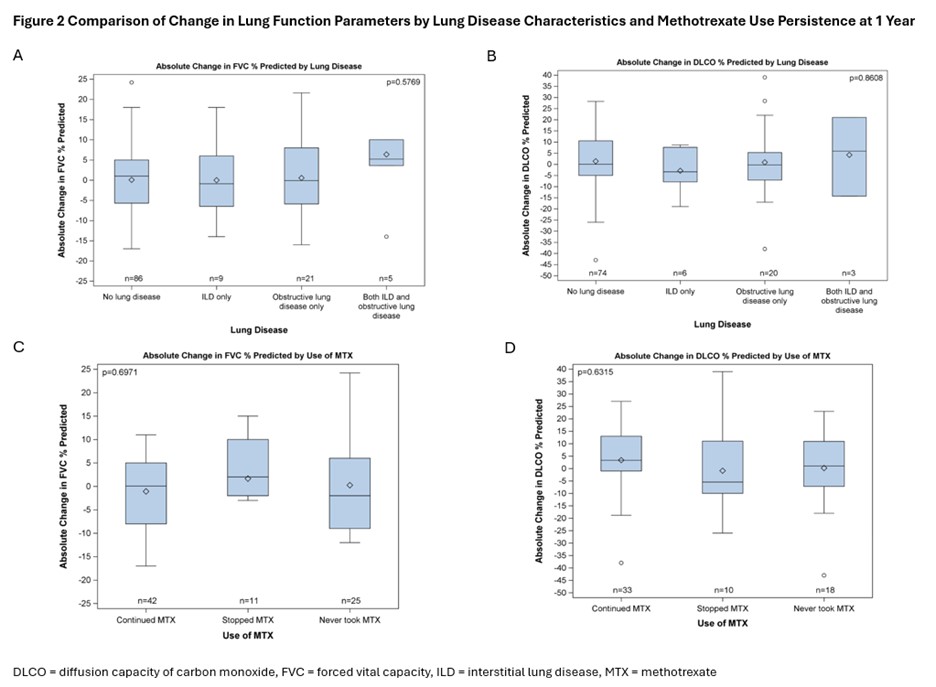
Background/Purpose: Several lung diseases are associated with rheumatoid arthritis (RA), including interstitial lung disease (ILD) and emphysema. In RA-ILD baseline lung function and decline in lung function may act as predictors of survival. We aimed to explore change in lung function over 1 year in cohort of participants with early RA. Methods: SAIL-RA (Study of Inflammatory Arthritis and ILD in Early RA) is a prospective, longitudinal, multicenter study of patients with RA within 2 years of RA diagnosis. Participants were enrolled from 2017 to 2025 at 5 U.S sites. We analyzed participants who completed baseline and 1 year assessments; including baseline high-resolution CT chest (HRCT) as well as pulmonary function tests (PFT) and disease activity assessment (DAS28-ESR) at both visits. We assessed changes in lung function by evaluating mean change in % predicted forced vital capacity (FVC) and diffusion capacity of carbon monoxide (DLCO) from baseline to 1 year using student’s T-test. We categorized participants into 3 groups based on change in PFTs (improved, stable, worsened). ‘Improved’ and ‘worsened’ FVC were defined as an increase or decrease of >5% predicted from baseline to 1 year. ‘Improved’ and ‘worsened’ DLCO were defined as an increase or decrease of >10% predicted from baseline to 1 year. We compared change in lung function based on baseline disease activity and presence/absence of ILD using Chi-square and Fisher’s exact tests. We compared distribution of participants with worsened, stable or improved lung function based on presence/absence of lung disease and continuation/discontinuation of methotrexate (MTX) in baseline MTX users by ANOVA. Low and moderate/high disease activity were defined as DAS28-ESR of <3.2 and >3.3. ILD was defined by radiologists’ interpretation of HRCT. Obstructive lung disease was defined as emphysema on HRCT or FEV1/FVC< 0.7. Results: 121 participants completed baseline and 1 year assessments with PFTs (Table 1). In the whole cohort approximately half of participants had worsened or improved FVC and/or DLCO at 1 year (Fig 1). The percentage of participants with worsened, stable, or improved FVC was 27.3%, 46,3%, and 26.4%. For DLCO 12.6%, 65%, and 22.3% had worsened, stable, or improved values. In participants with ILD versus no ILD at baseline there was a trend toward worsened FVC % predicted at 1 year in participants with ILD (p=0.089), although mean absolute change in FVC did not differ (2.26% vs 0.16%, p=0.44). There was no difference in the change FVC or DLCO % predicted from baseline to 1 year based on presence or absence of lung disease nor MTX continuation at 1 year (Fig 2). In participants with low versus moderate/high disease activity at baseline there was no difference in distribution of improved, stable or worsened FVC or DLCO at 1 year (p=0.54, p=0.21). Conclusion: In this prospective cohort of participants with early RA mean change in the FVC and DLCO at a population level was small, although there was significant individual variability over 1 year. While about 20% had worsened FVC or DLCO, most were stable or improved. There was a trend towards a higher proportion of participants with ILD to have worsened FVC compared to those without ILD. MTX use over 1 year was not associated with changes in FVC or DLCO.